Classification
Kuru is an always infections prion disease and is one of five known Transmissible Spongiform Encephalopathies (TSE) that have been found in humans. Prion diseases such as Kuru do not have the same classification as normal microorganisms as they do not have a genus or species. Instead, they are classified based on their host species, clinical disease, and the phenotypes of their lesions.
Kuru causes amyloid plaques in the cerebellum which can be obtained from postmortem victims of the disease. These plaques can stain with Alican blue, Congo red and the Periodic Acid-Schiff method (Figure 1). Kuru also mostly affects the cerebellum of individuals causing progressive cerebellar ataxia. This sets Kuru apart from other prion diseases because it affects a different part of the brain (Figure 2).

Figure 2: Areas of the brain affected by prion diseases.
The Disease
Symptoms
- Slurred speech
- Lack of coordination
- Unsteady gait
- Crying or Laughing uncontrollably
- Paralysis
- Tremors
- Increased sensitivity to cold
Clinical Stages
Before the onset of actual symptoms, Kuru has a pronominal stage that usually includes headache and limb pain; primarily in the joints.
- Ambulant stage: Patient is unable to stand without being assisted. They have unsteady gait, lack of voluntary muscle coordination (ataxia), and shivering tremors starting in the upper body and amplified by cold. They often show titubation (nodding of the head) accompanied by other abnormal movements.
- Sedentary: This stage begins when the patient is unable to move without assistance. Patients cannot maintain their posture, ataxia becomes severe, more tremors and enter into dysarthria.
- Terminal: Bedridden stage. Patients only have primitive reflexes and have dysphasia. Patients in this stage usually die due to starvation or pneumonia.
Specific Pathology
Kuru primarily infects the cerebellum of individuals, and only infects nervous tissue. It begins it's infection by being ingested into the body. From there it can exit the intestinal wall and find it's way to the lymph nodes where it remains until being picked up by peripheral nerves. Kuru then remains in the nervous tissue, as that is the only place it can reproduce. Neurons infected by Kuru are shrunken, hyperchromic or pale. Excessive amounts of vacuoles can be seen in the purkinje cells of the cerebellum, striatum and other neurons. These cells area said to look 'moth eaten.' Purkinje cells are often found missing, which shows the spongiform characteristics of Kuru. Some infected purkinje cells can be observed to have torpedo formations within them. The most severely affected tissue is the Paleocerebellum. The individual exits the Ambulant stage when Kuru causes more tissues in the cerebellum to die. Attacking the nervous tissue causes proliferation of astroglial and microglial cells. The microglial cells are primarily macrophages which cause an abundance of neuronophagia. The spinal cord is also infected primarily in the corticospinal and spinocerebellar tracts. Myelin degeneration also often happens in victims of Kuru, which slows impulses. The amyloid plaques mentioned earlier in the website are most often seen in the cerebellum, basal ganglia, thalamus and cerebral cortex respectively. Kuru has long incubation periods, and may not show any of these signs until up to 14 years after exposure, but normally Kuru presents itself within 4-6 years. Death normally happens as a result of these effects within 1 year, but can last as long as 23 months.
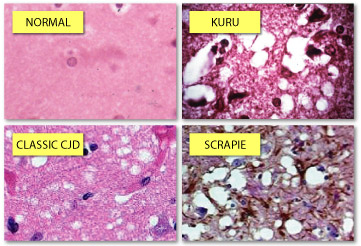
Figure 1: Phenotypes of Prion Lesions
Biology
Transmission
Kuru has only been found within Papua New Guinea; primarily within the Fore tribe. This is because you can only get Kuru by eating the infected tissues of somebody already affected, and the Fore people mourned their dead through ritualistic cannibalism.
The Prion Hypothesis
The Prion Hypothesis is that prions turn normal proteins within nerves known as PrP^c into misfolded proteins known as PrP^sc. These PrP^sc proteins cause chain reactions within nervous tissue turning nearby PrP^c protiens into more infectious PrP^sc prions. These prions then can stick together forming plaques that will kill the nervous tissue infected, but leave the plaque. This causes the observable spongiform effects in the brain as holes are created where there should be nerves (Figure 1). Converting host PrP^c into PrP^sc is how Kuru and other TSE diseases reproduce.These prions then can stick together forming plaques that will kill the nervous tissue infected, but leave the plaque. This causes the observable spongiform effects in the brain as holes are created where there should be nerves (Figure 1).
Treatment
There is no treatment or cure for Kuru as it is very hard to kill. Some experiments even show Kuru prions surviving after sitting in formaldehyde for decades. With that, the only measures that can be taken to treat Kuru are preventative and supportive. The preventative being discouraging the practice of cannibalism. This has shown to be effective in preventing further deaths from Kuru after the Fore people stopped cannibalistic practices in the 1950s. Supportive measures include people helping Kuru patients move and eat. Other supportive measures could include antidepressants and therapy; as many Kuru patients become silent in early stages because they understand they will die within a year.
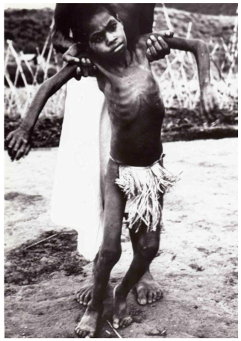
Figure 3: A victim of Kuru in the Sedentary Stage